ARA/Controlled Arch Orthodontics
Orthodontics is more than just straight teeth
Many dentists and orthodontists treat only crowded and misaligned teeth, and don’t treat the underlying cause. Controlled Arch Orthodontics can.
What is the most common underlying cause for malocclusion?
An underdeveloped upper jaw. Upwards of eighty percent of the modern population has an underdeveloped upper jaw and midface when comparing it to population groups not eating a modern diet and not exposed to modern pollutants. When the upper jaw is underdeveloped, the lower jaw is often retruded causing compression of the jaw joints, a decreased airway capacity, incorrect cervical spine alignment, poor body posture, and of course teeth misalignment.
How does this occur?
The most important requirement of the human body is air. Without air we live only a few minutes, and because of this we have a physiological airway, the nose, and an emergency airway the mouth. If you can’t or don’t breathe through your nose, you become a habitual mouth breather which has the tongue not properly positioned lightly suctioned to the palate. When mouth breathing becomes the norm, the upper jaw remains narrow and grows vertically downward. Just as the upper jaw development occurs because of nasal breathing, the lower jaw size and shape is a result of the upper jaw.
With an underdeveloped upper jaw, the lower jaw is constricted to develop inside the lower jaw which results in crowding, the jaw being trapped in a posterior position, compression of the jaw joint, and a decreased size of the airway. Many people over time will develop TMD and/or Obstructive Sleep Apnea. People with severe sleep apnea are 4 times more likely to die of any cause than someone else their own age without sleep apnea, and 5 times more likely to die from a heart attack or stroke.
Development and growth of the upper and lower jaws occurs between ages 6-13 years. The jaws between these ages should be stimulated by the proper tongue position on the palate which stimulates a nerve for forward upper jaw growth. and swallowing movements to stimulate the jaws to grow forward. Face forward growth is natural, healthy, physiological, and associated with beauty!

Face Forward Growth

Vertical Growth
How can we fix underdeveloped Jaws?
There are several techniques available today that can correct the foundation that is missing in adulthood due to the underdevelopment of the jaws. These appliance therapies for adults stimulate gently and safely the lifelong physiological cellular remolding potential in both the jaws and face. By applying the proper force, we can create space for crowded teeth, move the teeth of the upper jaw forward, and allow the lower jaw to also move forward. These changes improve the appearance of the nose, cheek bones, eyes and improve the jawline. This also improves the stability of the cervical vertebrae, especially C1 and C2, and increase the volume of the airway, and improve nasal breathing.
These methods include:
- Anterior Remodeling Appliance (ARA)
- Daytime Nighttime Appliance (DNA)
- Controlled Arch Braces
- Myofunctional Therapy
- Neuromuscular Dentistry
Will I need jaw surgery or extractions?
For many years, dental bite problems were remedied by two methods. The first was extracting teeth. In a crowded mouth, removing teeth in an already underdeveloped jaw, and making it even smaller only increases potential problems. Once the teeth are extracted, the front teeth are moved or retracted backwards to close the space. The second method was an expensive and risky jaw surgery to reposition one or both jaws. Both of those methods are not physiological and may take years and can be quite painful. In our practice our philosophy of orthopedics and orthodontics means no jaw surgery and no extractions.
It is never too late to treat patients with an underdeveloped maxilla. Expansion of the dental arches is widely practiced by dentists and orthodontists, but most do not expand anteroposteriorly (maxillary advancement). Maxillary advancement will create more space for the tongue and will facilitate improvement in the airway, TMJ pain, and aesthetics, including a person’s profile.
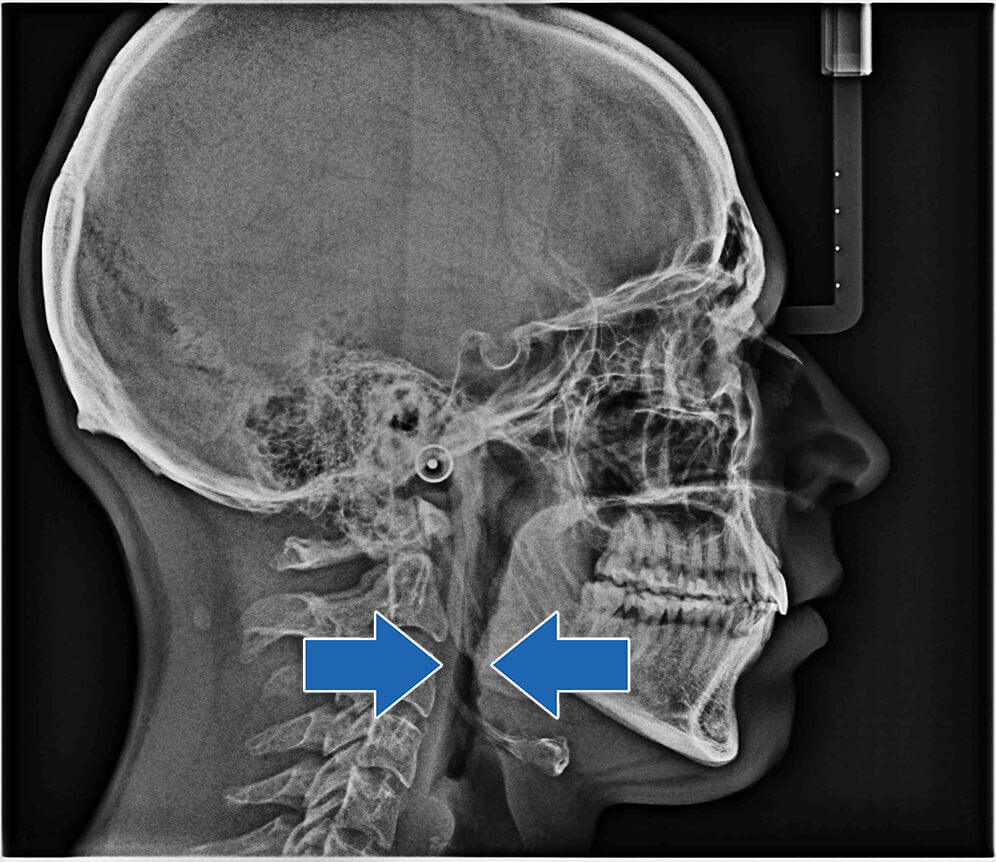
Before
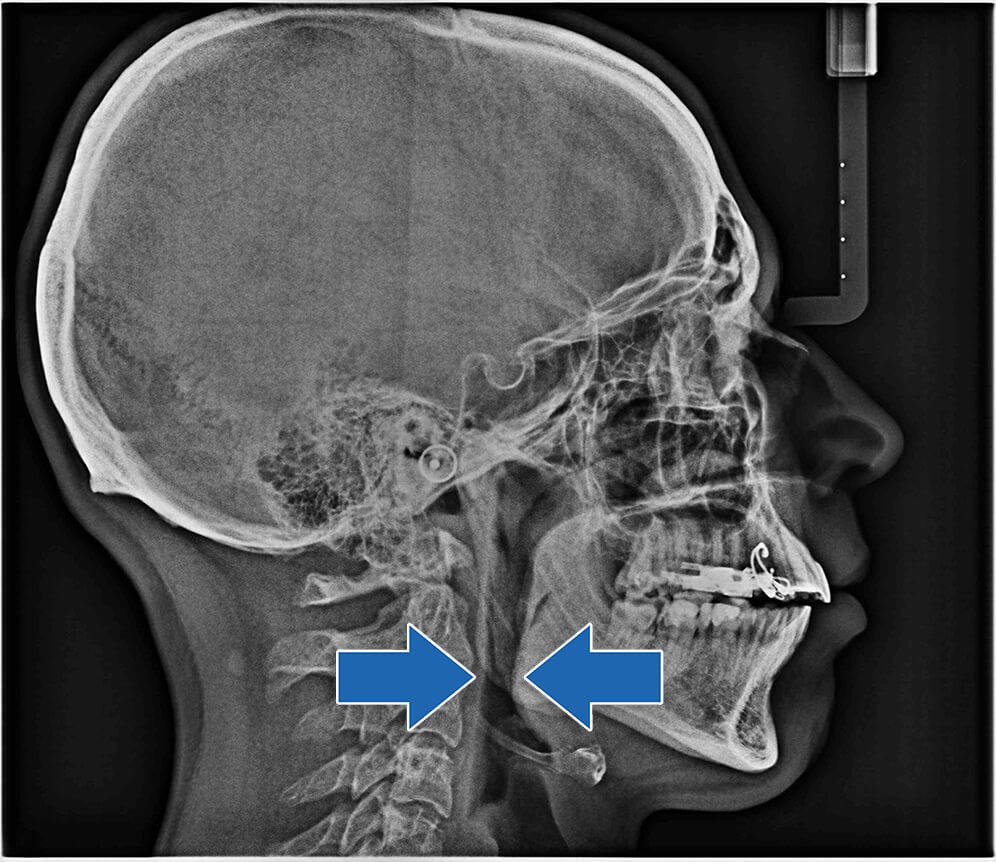
3 Months ARA
Fixed Anterior Remodeling Appliance (ARA)
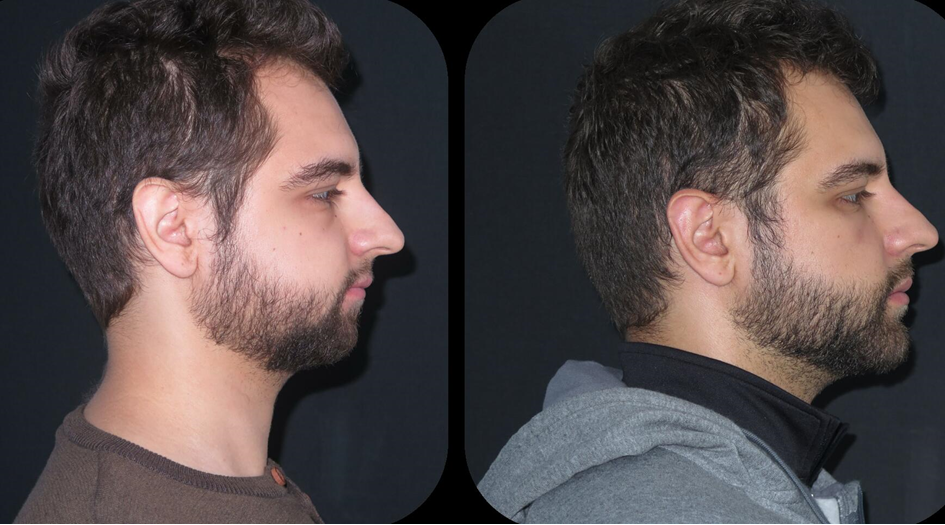
The fixed ARA is designed for patients with an adult dentition which is typically around 12 years of age, who have severely underdeveloped maxillary jaws. The fixed ARA cannot be taken out and expands the upper arch anteriorly (forward). Once the desired space is created the appliance is removed and Controlled Arch Orthodontics is commenced. ARA stimulates 3-dimensional face corrections improving asymmetry and balance. Moving the upper jaw forward allows the lower jaw to freely move forward and remodel to make a profound profile change like the photos below which took 4-7 months to achieve.
Before and After Photos from ARA Treatment



What is Controlled Arch Orthodontics?
It is a straight wire orthodontic system and technique of specific wires, stop locks, elastics and FRLA’s (Fixed Removable Lingual Arch wires). It looks like conventional orthodontics, but its mechanics are not. Controlled Arch has excess arch wire that exerts force anteriorly and laterally to develop the arches. Because the teeth are moved while maintaining the developed bone, the arch is “controlled. “Controlled Arch can be used alone as the only orthodontic treatment to create forward jaw movement and beautiful wide U-shaped arches, or as a “Phase II” treatment option following a DNA or ARA appliance therapy.
What is the difference between Conventional and Controlled Arch Orthodontics?
Controlled Arch is
PROTRACTIVE Orthodontics
Versus
Conventional Orthodontics is
RETRACTIVE Orthodontics
Controlled Arch Orthodontics is physiological.
- Jaw development is 3 dimensional and precedes movement of the teeth.
Conventional Orthodontics is mechanical.
- The teeth are moved within the confines of the existing jaws.
- Jaw development is 2 dimensional and occurs with tooth movement.
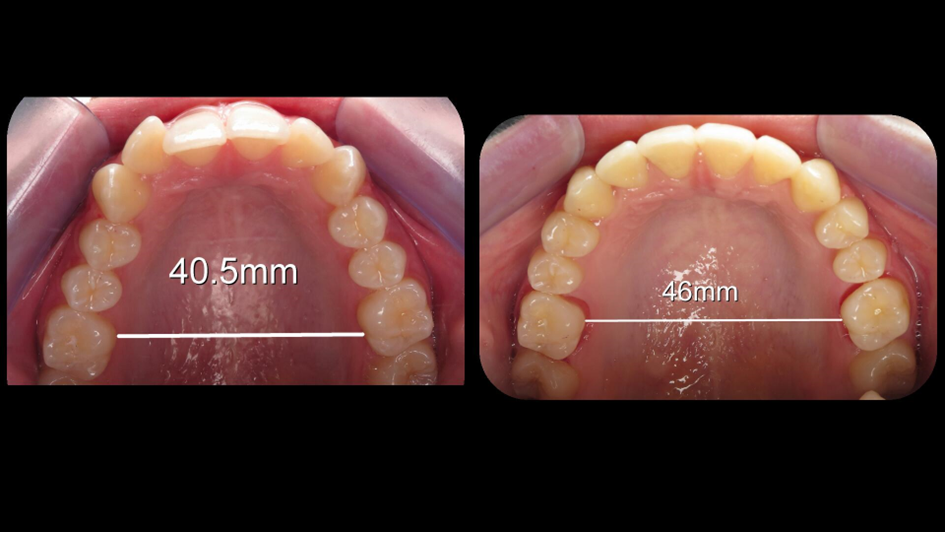
The result of Controlled Arch Orthodontics is the complete upper jaw being advanced forward by a few to many millimeters, and both jaws being expanded laterally in width. Both arches occlude into ideal bite harmony with the TMJ joints and the facial muscles. The result is an enlarged space in the mouth that allows the tongue to position itself in the roof of the mouth and allowing proper swallowing patterns. The more anteriorly positioned upper and lower jaws are, the larger the airway space will be which improves breathing capacity and decreases risk of Obstructive Sleep Apnea.
Before and After Controlled Arch Photos



What can I expect from facial growth orthodontic treatment?
The goal is to create the environment that the oral facial structures re-establish proper working function and esthetics. This proper function will create a physiological relationship between the muscles, joints, and jaws, along with cervical vertebrae and the airway to be healthy and pain free for life. To achieve this goal, 3 important changes need to occur which will be imperative in achieving good treatment success and a lasting dental occlusion that does not relapse.
- Return mouth breathing to nasal breathing.
- Teach proper lip seal.
- Train proper tongue and oral posture.
Before treatment commences, we also assess the airway and determine if there is any airway obstruction. If so, we refer to an Ear Nose Throat Doctor (ENT) for treatment. Patients with allergy problems will be sent to an allergist and patients with dysfunctional tongue habits will be referred to a myologist.
Do I need facial growth orthodontic treatment?
We will need to do an exam and take a series of photographs, X-rays and intra oral measurements to determine the position of the upper jaw and whether it is midface deficient or not. Patients with a midface deficiency will be recommended the appropriate treatment, and if there is only mild or no midface deficiency, only myofunctional therapy may be recommended.